
Podcast: Play in new window
Subscribe: RSS
Date: October 14th, 2020
Guest Skeptic: Dr.Salim Rezaie is a community emergency physician at Greater San Antonio Emergency Physicians (GSEP), where he is the director of clinical education. Salim is probably better known as the creator and founder of the wonderful knowledge translation project called REBEL EM. It is a free, critical appraisal blog and podcast that try to cut down knowledge translation gaps of research to bedside clinical practice.
Reference: Rowell et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA 2020.
Case: A 42-year-old helmeted bicycle rider is involved in an accident where he hits his head on the ground. At the time of emergency medical services (EMS) arrival, the patient is alert but seems a bit confused. The accident was within one hour of injury and his Glasgow Coma Scale (GSC) score was 12. Vital signs show a slight tachycardia but otherwise normal. Pupils were both equal and reactive and he doesn’t appear to have any other traumatic injuries, or focal neurologic deficits. Other injuries appear minimal with some abrasions from the fall.
Background: The CRASH-2 trial, published in 2010, showed a 1.5% mortality benefit (NNT 67) for patients with traumatic hemorrhage who received tranexamic acid (TXA) compared to placebo. Dr. Anand Swaminathan and I covered that classic paper on SGEM#80.
TXA has become standard practice in many settings as a result of this data. However, patients with significant head injury were excluded in this study and it was unclear of the effect of TXA in this group.

CRASH-3
Fast forward to October 2019, when CRASH-3 was published. This large, very well-done randomized placebo-controlled trial examined the use of TXA in patients with traumatic brain injuries (TBIs) with GCS score of 12 or lower or any intracranial bleed on CT scan and no extracranial bleeding treated within 3 hours of injury. The authors reported no statistical superiority of TXA compared to placebo for the primary outcome of head injury-related deaths within 28 days. We reviewed that article published in the Lancet in SGEM#270.
Subgroup analysis did demonstrate that certain patients (GCS 9 to 15 and ICH on baseline CT) showed a mortality benefit with TXA. While very interesting and potentially clinically significant, we need to be careful not to over-interpret this subgroup analysis.
We did express concern over the possibility that this subgroup would be highlighted and “spun”. Unfortunately, that did happen with a subsequent media blitz and a misleading infographic. Further data is clearly needed to elucidate the role of TXA in patients with TBI.
Clinical Question: Does pre-hospital administration of TXA to patients with moderate or severe traumatic brain injury improve neurologic outcomes at 6 months?
Reference: Rowell et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA 2020.
- Population: Patients 15 years of age or older with moderate or severe blunt or penetrating TBI. Moderate to severe TBI was defined as a GCS 3 to 12, at least one reactive pupil, systolic blood pressure ≥90mmHg prior to randomization, able to receive intervention or placebo within two hours from injury, and destination to a participating trauma center.
- Exclusions: Prehospital GCS=3 with no reactive pupil, start of study drug bolus dose greater than two hours from injury, unknown time of injury, clinical suspicion by EMS of seizure activity, acute MI or stroke, or known history, of seizures, thromboembolic disorders or renal dialysis, CPR by EMS prior to randomization, burns > 20% total body surface area, suspected or known prisoners, suspected or known pregnancy), prehospital TXA or other pro-coagulant drug given prior to randomization or subjects who have activated the “opt-out” process.
- Interventions: They had two intervention groups.
- The Bolus Maintenance Group received an out-of-hospital TXA 1g intravenous (IV) bolus and in-hospital TXA 1g IV 8-hour infusion.
- The Bolus Only Group received an out-of-hospital TXA 2g IV and in-hospital placebo 8-hour IV infusion.
- Comparison: The Placebo Group received Out-of-hospital saline IV bolus and in-hospital saline 8-hour infusion.
- Outcome:
- Primary Outcome: Favorable neurologic function at 6 months (defined as Glasgow Outcome Scale-Extended Score >4 which is considered moderate disability or good recovery)
- Secondary Outcomes: There were 18 secondary endpoints, of which 5 reported statistical analysis in this trial
- 28 day mortality
- 6-Month Disability Rating Scale Score (0 equals no disability and 30 equals death)
- Progression of intracranial hemorrhage (Defined as >33% increase in the combined volume of hemorrhage)
- Incidence of seizures
- Incidence of thromboembolic events
Authors’ Conclusions: “Among patients with moderate to severe TBI, out-of-hospital tranexamic acid administration within 2 hours of injury compared with placebo did not significantly improve 6-month neurologic outcome as measured by the Glasgow Outcome Scale-Extended.”
 Quality Checklist for Randomized Clinical Trials:
Quality Checklist for Randomized Clinical Trials:
- The study population included or focused on those in the emergency department. Yes and No
- The patients were adequately randomized. Yes
- The randomization process was concealed. Yes
- The patients were analyzed in the groups to which they were randomized. No
- The study patients were recruited consecutively (i.e. no selection bias). Unsure
- The patients in both groups were similar with respect to prognostic factors. Yes
- All participants (patients, clinicians, outcome assessors) were unaware of group allocation. Yes
- All groups were treated equally except for the intervention. Yes
- Follow-up was complete (i.e. at least 80% for both groups). Unsure
- All patient-important outcomes were considered. Yes
- The treatment effect was large enough and precise enough to be clinically significant. No
Key Results: They enrolled and randomized 1,063 patients with 966 patients included in the primary analysis group. The mean age was in the late 30’s, ¾ were male, the vast majority (>95%) of patients had blunt trauma, mean out-of-hospital GCS score was 8 and the mean time from injury to out-of-hospital study drug administration was just over just over 40 minutes.
No statistical difference in favorable neurologic function at 6 months with TXA compared to placebo.
- Primary Outcome: Favorable Neurologic Function at 6 Months
- 65% TXA groups vs. 63% Placebo group
- Difference 3.5% (90% 1-sided confidence limit for benefit, −0.9%); P = 0.16
- Secondary Outcomes:
- 28 Day Mortality: No statistical difference between groups (14% vs. 17%)
- Disability Rating Scale Score: No statistical difference between groups (6.8 vs. 7.6)
- Progression of Intracranial Hemorrhage: No statistical difference between groups (16% vs. 20%)
- Incidence of Seizures: Bolus Only (5%), Bolus Maintenance (2%) and placebo (2%). Not statistically significant.
- Thrombotic Events: Bolus Only (9%), Bolus Maintenance (4%) and placebo (10%)

1. Survival Bias: When a selection process of a trial favors certain individuals who make it past a certain point in time and ignores the individuals who did not. In other words, patients who die shortly after the start of follow-up may not have had an opportunity to become exposed and will not have their results recorded. This introduces an artificial survival advantage associated with the exposed subjects regardless of treatment effectiveness. When survivor treatment selection is not addressed, ineffective treatment may appear to prolong survival or worsen adverse events. Severely injured patients who survive longer in the bolus only group may have lived long enough to experience more complications and only those who survive out to 6 months can have an outcome recorded.
2. Glasgow Coma Scale (GCS) Score: The GCS has limitations including inter rater reliability (IRR) issues. This could have contributed to 20% of patients originally given a score of <13 in the pre-hospital setting arrived at the hospital with a GCS of 13 or greater. Another concern is that the GCS is not a diagnostic tool. It cannot reliably discriminate between CNS depressed states (intoxication, hypoglycemia, sedation, shock, seizure, etc) and intracranial hemorrhages.
3. Few Intracranial Hemorrhages (ICHs): This trial ultimately only had a small number of patients with ICH (58%). This means many patients without ICH were given TXA and were included in the analysis. While being practical it could dilute any potential treatment benefit of TXA in patients with isolated TBI.
4. Loss to Follow-Up: Depending on how you define and calculate loss to follow-up. It was at least 15% and could have been as high as 23%. I usually get concerned when the loss to follow-up is larger than the difference in the primary outcome. This is more important when the authors are claiming superiority which they are not doing in this case. The authors correctly do not conclude superiority but that does not mean we should conclude TXA given pre-hospital does not work in patients with isolated TBI. However, this trial does not support that TXA does work but, given the limitations we have discussed, it is still a reasonable hypothesis that it may work and merits further testing.
5. Minimal Clinically Important Difference (Statistical vs Clinical Significance): Although the study was not powered to detect a difference in mortality (secondary outcome), in this trial we see a ≈3.0% difference in 28-day mortality (not statistically significant) which could be clinically important at a population level. If we assume an estimated 56,000 TBI-related deaths per year in the US, then a 1% difference could decrease mortality by ≈560 cases per year in the US. If we use the ≈3.0% in this study, that would decrease mortality by 1,600 cases per year in the US. Of course, that all depends on “if” this is a true effect of TXA in these patients.
Comment on Authors’ Conclusion Compared to SGEM Conclusion: We generally agree with the authors’ conclusions.
SGEM Bottom Line: The routine use of TXA in the pre-hospital setting for patients with isolated moderate or severe TBI cannot be recommended at this time.
Case Resolution: After evaluation of the patient it is decided to not administer TXA prehospitally as the patient has an isolated TBI, no other traumatic injuries that would benefit from TXA and the lack of robust evidence to support its use in TBI in the out-of-hospital setting.

Dr. Salim Rezaie
Clinical Application: This trial of TXA vs placebo given within 2 hours of injury, in the out-of-hospital setting, in patients with moderate or severe traumatic brain injury (GCS ≤ 12) combined with the results of the CRASH-3 (SGEM#270) and the TICH-2 trial (SGEM#236), we have no high-quality evidence to support the routine use of out-of-hospital TXA in patients suspected of having ICH.
What Do I Tell My Patient? You have had a head injury. We would like to admit you to the hospital for observation, neurologic checks, and ensure there are no changes over the next 24 to 48 hours. The CT scan we performed did not show any bleeding in the brain.
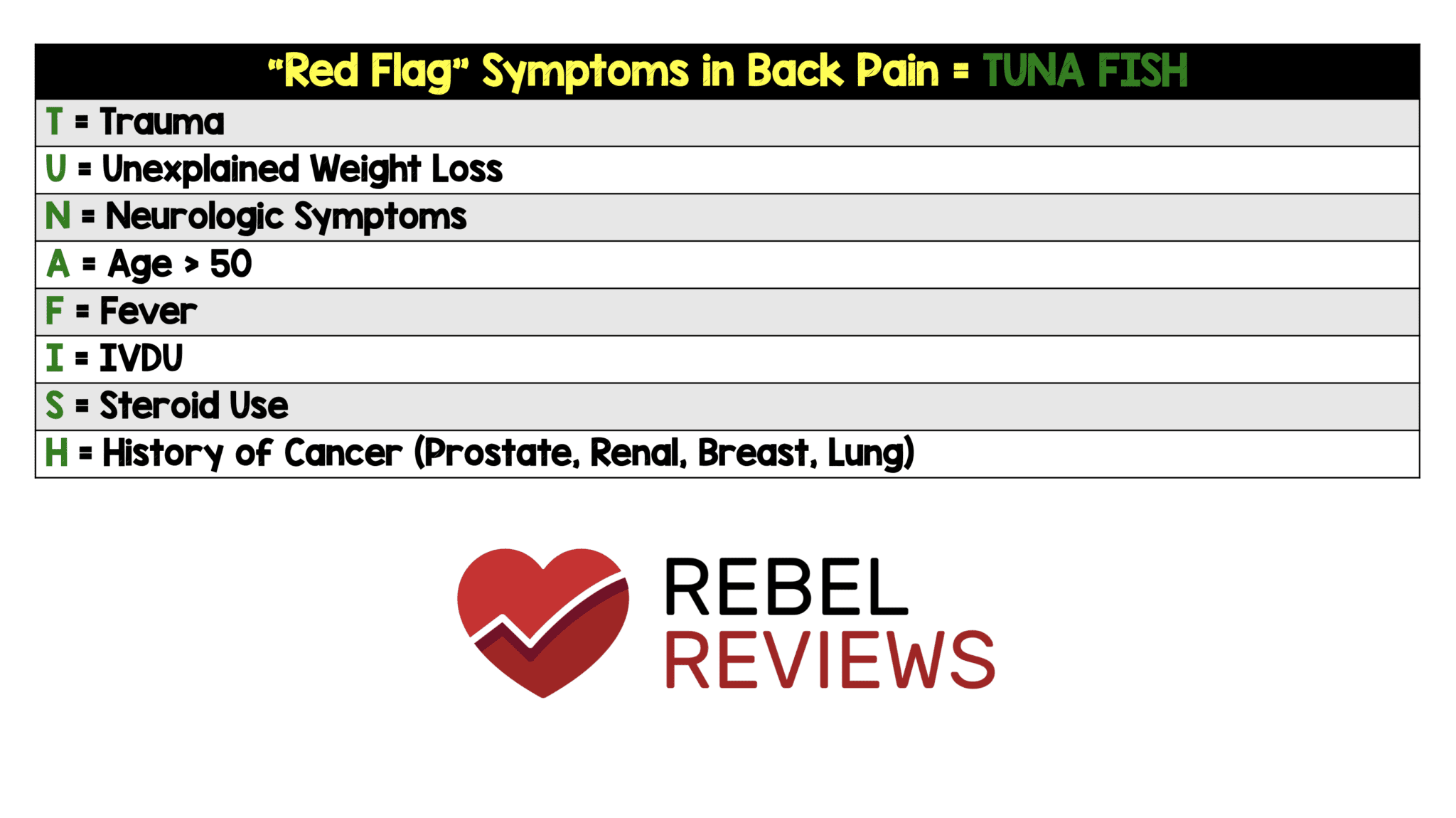
Keener Kontest: Last weeks’ winner was Dr. Daniel Mirsch a Clinical Assistant Professor University at Buffalo. He knew TUNAFISH is a mnemonic to remember the red flags of low back pain.

Listen to the SGEM podcast to hear this weeks’ question. Send your answer to TheSGEM@gmail.com with “keener” in the subject line. The first correct answer will receive a cool skeptical prize.
Other FOAMed:
- EM Lit of Note: TXA, The Miracle Drug With Mostly Negative Trials
- REBEL EM: CRASH-3 – TXA for ICH?
- Emlyn’s: TXA in Severe Head Injury




{kind=link}
{kind=link}
You must be logged in to post a comment.